


















Healthcare systems around the world have been required to adapt to deal with the coronavirus pandemic. While some countries have been able to continue working almost as normal, others have seen systems and hospitals overwhelmed. With these challenges, systems, hospitals and medical staff have had to change the way they work, often dramatically. There has been a period of introspection across society, and what seemed important before now appears irrelevant, and changes that were resisted before having now been happily accepted. With this backdrop, how has the management and treatment of patients with arrhythmias changed?
Virtual clinics and video calling have become an accepted part of the way we work now, and the resulting rise of remote and wearable diagnostics has been dramatic. The use of devices such as the Apple Watch and other wearable ECG monitors have moved considerably into the mainstream and are likely to yield an even higher number of patients requiring medical expertise and treatment. In many ways, electrophysiologists can adapt easily as we lean towards the ECG as our main diagnostic tool when physical examination is restricted. However, direct face-to-face contact is now harder to achieve, and the control of quality information to patients is as important as it ever has been.
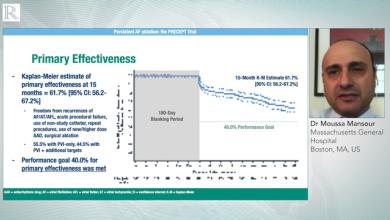
Interventional treatment of arrhythmias, in particular AF, while a relatively mature technique still has unanswered questions. As a community we have often focused on the underlying mechanism or trying to understand different forms of signal analysis. While process improvements were discussed, they were rarely the primary focus. In the current situation, with more limited access and time, the way in which we treat patients is much more important. Having patients in hospital for the least amount of time possible is now a priority. This has a number of important implications in the management of patients with AF. Whereas trial endpoints of mortality and stroke reduction were seen as a gold standard, perhaps more emphasis should be placed on endpoints such as reduction in hospital admissions and outpatient visits.
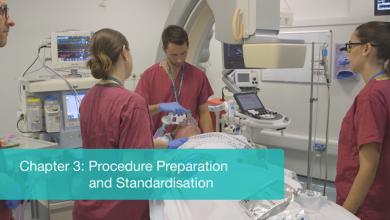
Day-case AF ablation has been the standard in many hospital units for a number of years, regardless of what technology has been employed. However, this has been resisted in many healthcare systems with both medical and financial reasons often cited. Now, it seems inevitable that day-case AF ablation will become the standard of care.
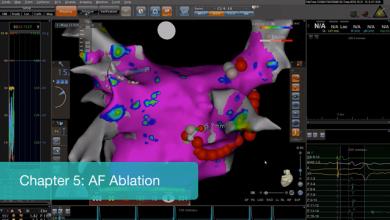
What other parts of the process can yield benefits by minimising the total time of the procedure? Single-shot devices are attractive, but standard point-by-point radiofrequency ablation has become much quicker, due to the standardisation of lesions, and a greater acceptance of high-power, short duration delivery. Again, this has been used in a number of labs for many years successfully, yet perhaps has not gained the respect and uptake that it should have done.
Standardisation of the process, tools that allow quicker lesion delivery, (including very high-power delivery) and electroporation will make AF ablation a shorter procedure and is likely to improve success rates. With this, will it be time to offer AF ablation sooner in a patient's journey, rather than waiting for medication failure, or repeated cardioversions? There will always be options for individual patients, but will the standard become interventional first rather than medication?
The website content and design has recently been updated and will allow for easier navigation. More content is being developed looking specifically at how we can improve the care of patients with arrhythmias in this new environment, not just maintain previous standards. Hopefully, we shall all be able to look back and find that the "new normal" has actually led to practice improvements.
Dr Matt Wright